To be enrolled in short term coverage the contract holder must be a resident of the state of Alabama not enrolled in Medicare or Medicaid and not currently on a short term limited duration plan. Be available until the next annual open enrollment or special enrollment period.
Https Www Bluecrossnc Com Document Group Dental Enrollment Application
Containing the billing entity information.

Bcbs enrollment application. I represent that the statements on this application are true and complete to the best of my knowledge and belief. Both companies are. Enrollment Department which will then submit your form to.
When submitting this enrollment application please be sure to include a completed W9. Forms for Facility Provider Enrollment Tutorial - Facilities can learn how to join the Blue Cross provider networks by viewing this web-based training. Box 3283 Tulsa OK 74112-3283 or via fax at 918-551-3179.
Please select which networks you wish to join. It can take us up to 90 days to review your enrollment application. Visit our external provider portal.
SECTION 9 Sign your name and date the enrollment application if you agree to the conditions set forth in this section. 1218 Provider Enrollment Application. 46 rows Mail or fax the completed form to BCBSIL see address and fax number at the top of the.
Enterupdate your information in CAQH EnrollHub. For a copy of the W9 and other instructions for this application. This enrollment applicationchange form.
Manually Submit Your Application Facilities must use this option when completing an application If youd rather email fax or mail your information youll need to fill out the application and send your documents to us. Enter the first three letters of the Identification Number from your member ID card. Explore resources benefits and eligibility requirements.
Enrollment does not establish you or your practice as an in-network BCBSNC provider. For information about premiums benefits and limitations and exclusions for short term plans please review the Benefit Booklet for Short Term Blue. Go to CAQH to Start Application.
Your enrollment application should be submitted to your employers Enrollment Department which will then submit your form by mail or email to. As a current member you can access your benefits and services from your local Blue Cross Blue Shield company. Blue Cross and Blue Shield of Oklahoma P.
STEP 2 Submit a signed contract. Please complete this application and submit it along with the other required documentation to. And requests for network participation.
BCBSTX Group Accounts Dept. GHS Health Maintenance Organization Inc. Once it is confirmed that you meet eligibility requirements BCBSIL will send you a contract via email for participation in the provider networks for which you qualify.
Enterupdate your information in CAQH ProView. This Provider Application will be used for assigning a provider number for Blue Cross and Blue Shield of Florida Inc. View a sample BCBS member card.
Download them fill out the PDFs electronically then print them and fax them to us. GrpMbrBenefitsApp3 APPLICATION TO ENROLL OR CHANGE ENROLLMENT Dependable Health Care Coverage from the Capital BlueCross Family of Companies Health care benefit programs issued or administered by Capital BlueCross andor its subsidiaries Capital Advantage Insurance Company Capital Advantage Assurance Company and Keystone Health Plan Central. Dba BlueLincs HMO is a wholly-owned subsidiary of Health Care Service Corporation a Mutual Legal Reserve Company.
Your enrollment application should be submitted to your employers. These forms and your required documents make up your enrollment application. Sign your name and date the enrollment application if you agree to the conditions set forth in this section.
BlueCross BlueShield of South Carolina and BlueChoice HealthPlan are independent licensees of the Blue Cross and Blue Shield Association. Apply online to be an Anthem healthcare provider. Please review the Facility Enrollment Required Document Checklist PDF for your classification type and ensure that you have all the needed information readily available to avoid processing delays.
Youll receive a letter to let you know that you have successfully enrolled. PO Box 655730 Dallas TX 75265-5730. Sign your name and date the enrollment application if you agree to the conditions set forth in this section.
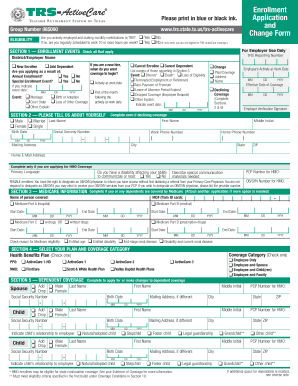
Andor Health Options Inc. I acknowledge that if I apply for Florida Blue Florida Blue HMO andor Truli for Health coveragemembership later coveragemembership may not. Group Enrollment Application Change Form.
Independent licensees of the Blue Cross and Blue Shield Association. If BlueCross BlueShield receives the enrollment application between the dates of January 16 2021 through January 31 2021. If BlueCross BlueShield receives the enrollment application between the dates of December 16 2020 through January 15 2021 coverage will begin February 1 2021 as long as the applicable premium payment is received by then.
Register with Availity complete your enrollment application or change form. Your enrollment application should be submitted to your employer who will then submit your form to. Please follow the instructions carefully and provide current.
Provider Application For use by Physicians and Independent Health Care Professionals PURPOSE. Heres where youll start to enroll as a new provider or add a provider to your group contract.
Https Www Bsc Edu Administration Humanresources Pdfs Benefits Health Bcbs 20enrollment 20form Pdf
Https Www Bcbstx Com Pdf Forms Grp Health Enroll App Tx 2017 Pdf
Https Www Bcbstx Com Pdf Forms Grp Health Enroll App Tx 2017 Pdf
 Fillable Online Blue Cross Blue Shield Texas Fillable Enrollment Form Fax Email Print Pdffiller
Fillable Online Blue Cross Blue Shield Texas Fillable Enrollment Form Fax Email Print Pdffiller
Https Wellesleyma Gov Documentcenter View 360 Bcbs Medex Enrollment Form Pdf
Https Www Bcbsnm Com Pdf Forms Grp Health Enroll App Nm 2016 Pdf
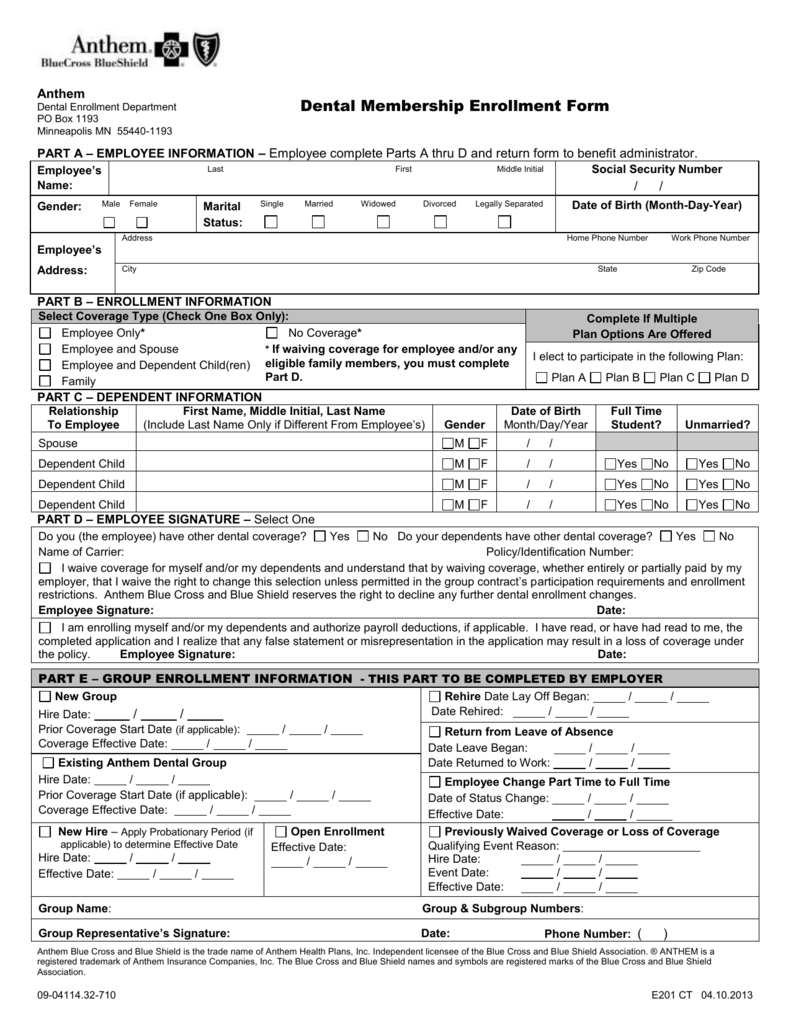 Membership Enrollment Form
Membership Enrollment Form
 Fillable Online Blue Cross Blue Shield Member Enrollment Application Group Size 2 99 Form Fax Email Print Pdffiller
Fillable Online Blue Cross Blue Shield Member Enrollment Application Group Size 2 99 Form Fax Email Print Pdffiller
Fillable Online Enrollment Application Form Pdf Blue Cross Blue Shield Of Fax Email Print Pdffiller
Https Www Bluecrossmn Com Sites Default Files Dam 2020 10 P11ga 25206604 2020 Enrollment Waiver Form F10936r02 Fill Pdf
Https Www Bcbsil Com Pdf Forms Grp Health Enroll App Il 2017 Pdf
Https Www Umass Edu Humres Sites Default Files Uma Pd Member Enrollment Form 0 Pdf
Https Www Empireblue Com Employer Noapplication F4 S2 T0 Pw B155593 Pdf Refer Ehpemployer
Https Www Amherst Edu System Files Media 0054 Bcbsma Member Enrollment Form Pdf
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.