Regular Medi-Cal FFS DoctorClinic Code. The SCCHA distinct from the County was given the mission to develop a community-based health plan Santa Clara Family Health Plan SCFHP to.
 Santa Clara Family Health Plan Picshealth
Santa Clara Family Health Plan Picshealth
Santa Clara Family Health Plan.
Santa clara family health plan authorization form. Choose one of these Medi-Cal Plans to get your Medi-Cal benefits. Effective immediately please be advised that the number to call 24hrs per day7 days per week is 18552548264. SCVMC is contracted with a number of health plans for outpatient services.
Anthem Blue Cross Partnrshp. Medi-Cal Preventable Conditions Reporting Form. PHC Medi-Cal TAR Form.
Authorization for Transportation Services and Physician Certification Statement. In 1995 the Santa Clara County Board of Supervisors established the Santa Clara County Health Authority SCCHA under the authority granted by Welfare and Institutions Code Section 1408736. 20 reviews of Santa Clara Family Health Plan For the last three weeks Ive never been able to get a human on the phone.
The Provider Link is an online tool for accessing eligibility claims and other helpful resources. I left my name and phone number twice clearly and still have never received a call back. PA Criteria Table Effective 01-01-2021.
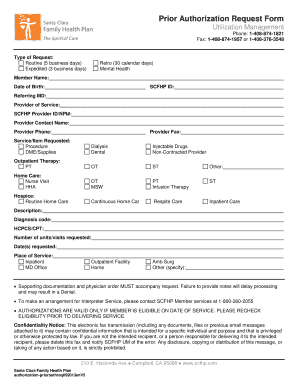
OPTION B Keep my Medicare the way it is now AND choose a Medi-Cal plan. In 2015 Santa Clara Family Health Plan the Plan launched Cal MediConnect to serve people in Santa Clara County who are eligible for both Medicare and Medi-Cal. This standard form may be utilized to submit a prior authorization request to a health plan for review along with the necessary clinical documentation to support the request.
Any call to any phone number other than 18552548264 does not constitute notice of patient admission or request for post stabilization care. Valley Health Plan VHP contracts with Primary Care Physicians PCPs and Plan Providers who are responsible to provide and coordinate Covered Services or Benefits for you the Member. Thank you for considering Santa Clara Valley Medical Center for your patients care.
Prior Authorization Supplemental Forms. Additional Health Plan Option- Program of All-inclusive Care for the Elderly PACE. Long-Term Care Discharge Notification Form.
Urgently needed care means services that are required in order to prevent serious deterioration of a members health that results from an unforeseen illness orinjury. Please take a look at our Outpatient Specialty Services and Contracted Health Plan pages for a complete list of services and plans. Forms Resources.
Echo Health - EFT and ERA 835 Enrollment Form. Post-stabilization care prior authorization. An accompanying reference guide provides valuable health plan specific.
309 Santa Clara Family HP. Login Username Password Submit Forgot your username or password. Validate and update your practice information.
Before you enroll refer to the Summary of Benefits for specific plan benefits. Post-stabilization care prior authorization request available 7 days a week 24 hours a day. Potential Quality of Care Issue PQI Referral Form.
VHP requires prior authorization for all post stabilization care. Santa Clara Family Health Plan Medicare-Medicaid Plan Location. I wish to JOIN or change my plan to.
Plan Partners KA KP Cal LLC 345 Anthem Blue Cross Partnrshp. Check status of claims. After being on hold several times each for 20 minutes or so and get disconnected.
ECOB Primary pharmacy claim information Hepatitis C Treatment TAR Information. Provider Dispute FormMultiple Like Claims. 408 937-3637 or 408 937-3638 Authorization Request Form Routine Non-Urgent Urgent.
Santa Clara Family HP. VEGF TAR Supplemental Form. 5 Applicants Name First Name Last Name 6 Sex.
Prior Authorization Forms. As of December 2018 Santa Clara Family Health Plan d 7695 Cal MediConnect members. 815 Santa Clara Family Health.
1-408-376-2000 TTY users 711. 2021 Medicare Advantage Plan Details. Request Health Education for Patient.
Summary of Benefits and Disclosure Form PDF Evidence of Coverage EOC PDF Summary of Benefits and Coverage SBC PDF. A fax about a patient admission or request for transfer does. Santa Clara Street Suite 950 San Jose CA 95113-1848 Phone.
1-408-874-1957 or 1-408-376-3548. Except in the case of Emergency Services Urgently Needed Services or if VHP has Prior Authorized services you must receive all of your care from these VHP Plan Providers. Twice after 20 minutes hold my call went to voice mail.
Plan Partner Name see back of choice form KA. H7890 - 001 - 0 Click to see other plans. 6a Due Date if pregnant 6b Social.
To learn more about member materials including forms please visit Santa Clara Family Health Plan SCFHP Forms Documents. Access PCP patient rosters. Check member eligibility and PCP status.
Enter plan change reason code. Authorization Form and accompanying reference guide. Download authorization request forms.
Https Res Cloudinary Com Dpmykpsih Image Upload Santa Clara Site 299 Media 1615 Pacpacket201811 Pdf
 Fillable Online Referral Authorization Form Raf Santa Clara Family Health Plan Fax Email Print Pdffiller
Fillable Online Referral Authorization Form Raf Santa Clara Family Health Plan Fax Email Print Pdffiller
2
 Santa Clara Family Health Plan Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Santa Clara Family Health Plan Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
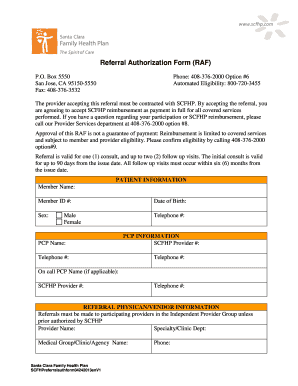 Fillable Online Scfhp Referral Authorization Form Raf Santa Clara Family Fax Email Print Pdffiller
Fillable Online Scfhp Referral Authorization Form Raf Santa Clara Family Fax Email Print Pdffiller
Https Www Scfhp Com Media 2743 2020 Eoc En Web Pdf
![]() Home Santa Clara Family Health Plan
Home Santa Clara Family Health Plan
Http Med Stanford Edu Content Dam Sm Ppc Documents Dbp Aba Gpchc Santa Clara Pdf
Https Res Cloudinary Com Dpmykpsih Image Upload Santa Clara Site 299 Media 1615 Pacpacket201811 Pdf
Https Www Scfhp Com Media 1575 Mc Eoc En Pdf
 Santa Clara Family Health Plan Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Santa Clara Family Health Plan Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
 Santa Clara Family Health Plan Authorization Form Fill And Sign Printable Template Online Us Legal Forms
Santa Clara Family Health Plan Authorization Form Fill And Sign Printable Template Online Us Legal Forms
Https Www Scfhp Com Media 2520 Authorizedrepform Eng Pdf
 Submit A Claim Or Dispute Santa Clara Family Health Plan
Submit A Claim Or Dispute Santa Clara Family Health Plan
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.