The 1095-B is quite similar to the 1095-A form. This form is available both in English and Spanish.
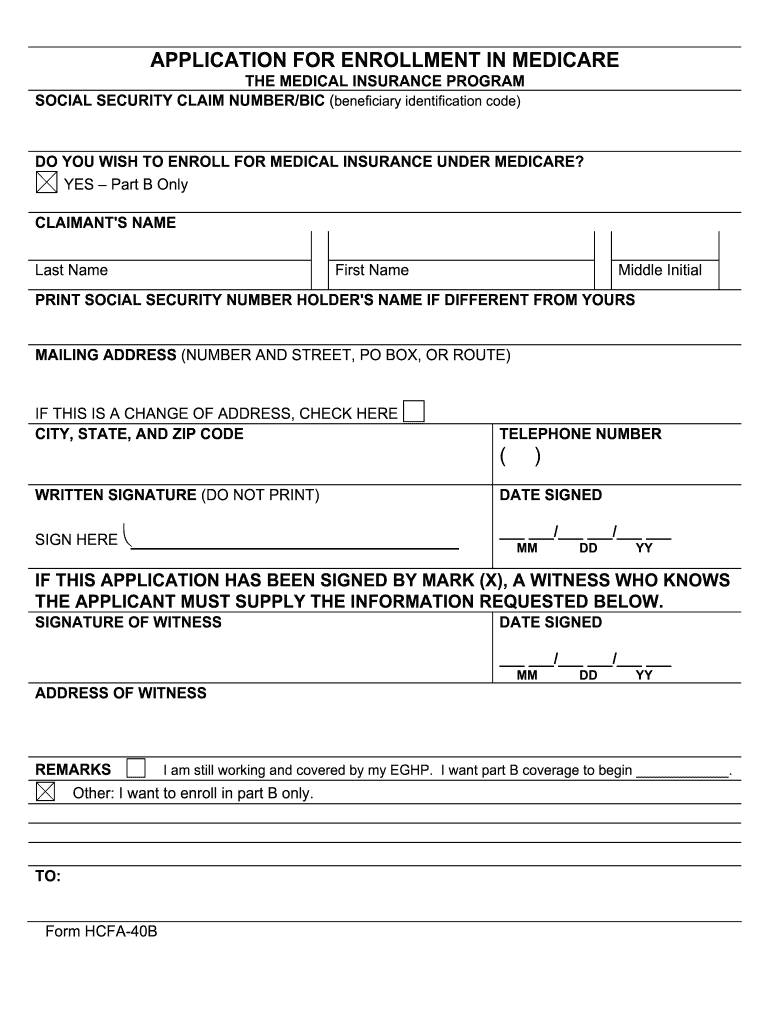 Form 40b Fill Online Printable Fillable Blank Pdffiller
Form 40b Fill Online Printable Fillable Blank Pdffiller
Part B also covers many preventive services.
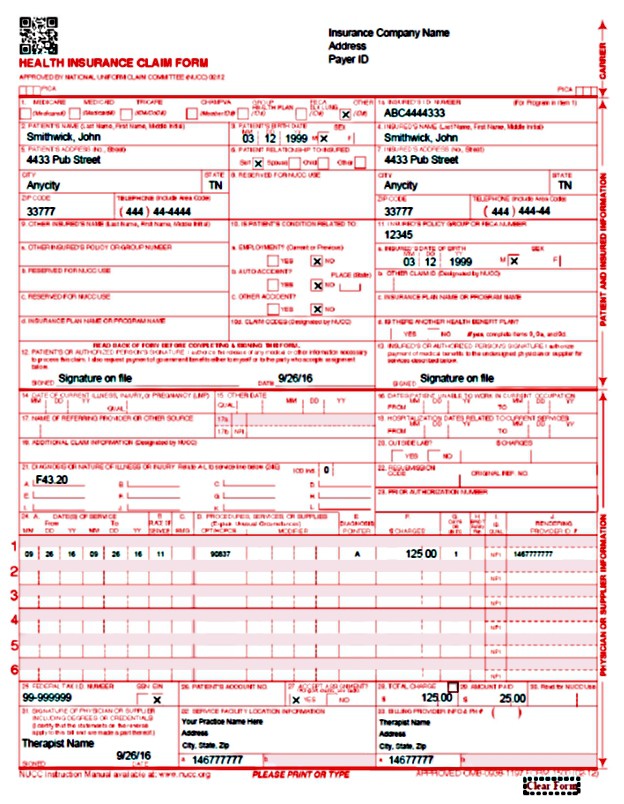
Medicare part a enrollment form. The following forms are routinely submitted with an enrollment application. CMS Form 1490S Patients Request for Medical Payment is a claim form that you can use to request payment for Medicare Part B covered services CMS Form 1490S Patients Request for Medical Payment is a claim form that you can use to request payment for Medicare Part B covered services. Fill out the Application for Enrollment in Part B CMS-40B.
Part B request for employer information. Go to Apply Online for Medicare Part B During a Special Enrollment Period and complete CMS-40B and CMS-L564. Live in the plans service area Important.
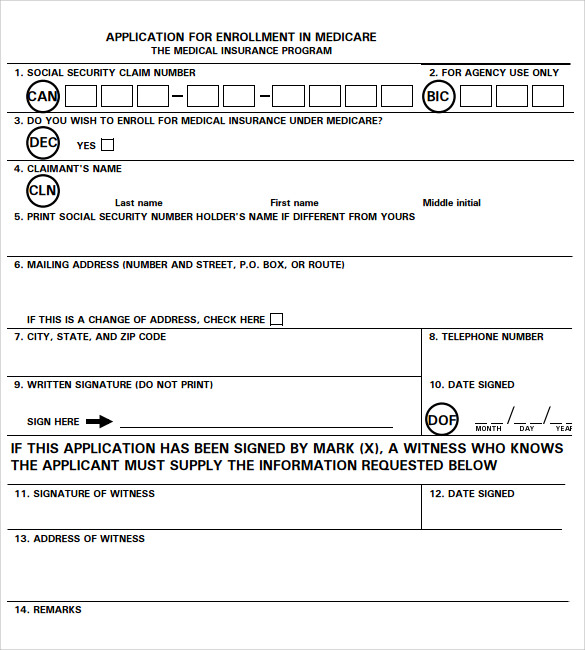
Medicare Part B Medical Insurance Part B helps cover medically necessary services like doctors services outpatient care and other medical services that Part A doesnt cover. The form requires your name claim number that is your Medicare ID number as it appears on your Medicare. Individual Enrollment Request Form.
Health Insurance Review Form. People with Medicare who want to join a Medicare Advantage Plan or Medicare Prescription Drug Plan. Printable and fillable Application for Enrollment in Medicare My Account Login.
Download and complete the Medicare enrolment form. You can use one of the following options to submit your enrollment request under the Special Enrollment Period. Electronic Funds Transfer EFT Authorization Agreement Form CMS-588 Medicare Participating Physician or Supplier Agreement Form CMS-460.
Scope of Appointment Form. Get the SF-5510 as a PDF form in Spanish or HMTL form in Spanish. This application is to sign up to get medical insurance under Medicare.
New Medicare Card Application Form in PDF. 2021 Medicare Part D or Medicare Advantage Plan Review Form. Be a United States citizen or be lawfully present in the US.
Medicare enrolment form MS004 Use this form to enrol in Medicare for the first time re-enrol in Medicare or enrol your baby in Medicare. If you have had your Medicare Card canceled in the past this is the best form to fill out to apply for a new one. Medicare Part B medical insurance.
If you dont have Part A and want to sign up please contact Social Security at. You and your referee need to fill in the Aboriginal and Torres Strait Islander Medicare enrolment and amendment form. Who can use this form.
You will receive the 1095-B form if you are enrolled in these programs. Be a United States citizen or be lawfully present in the US. If youre Indigenous and have common identity documents mail or email them with your Medicare enrolment form to Medicare Enrolment Services.
If your answer to this question is no then you dont need to fill out this application. If youre enrolled in a Medicare Advantage plan and wish to file a claim for Medicare-covered services or supplies that werent covered fill out a Patient Request for Medical Payment form and submit it to your health insurance company. IRMAA 2021 appeal document.
Part B coverage is your choice. It is also the right document to use if you know your Medicare Card has expired and you want to renew. To Enroll in a Medicare Advantage Plan Part C OMB No.
You can find this form on Medicaregov or contact Medicare directly. Remember to sign it before you submit it with your supporting documents. Social Security enrolls you in Original Medicare Part A and Part B.
If youre enrolled in Original Medicare Part A and Part B claims are handled by doctors and suppliers. 1-312-751-4701 Monday through Friday from 9AM to 330PM. This form if you already have Medicare Part A Hospital Insurance.
Go to your local Social Security office and ask to be enrolled in Medicare Part B. Medicare Part A hospital insurance helps pay for inpatient care in a hospital or limited time at a skilled nursing facility following a hospital stay. To join a plan you must.
Fax or mail your CMS-40B CMS-L564 and secondary evidence to your. CMS-20134 PDF for MDPP Suppliers. However you need to have Part.
INDIVIDUAL ENROLLMENT REQUEST FORM TO ENROLL IN A MEDICARE ADVANTAGE PLAN PART C Who can use this form. 2020 Agent of Record Anthem. Part A also pays for some home health care and hospice care.
Enrollment forms I have Part A and want to apply for Part B Application for Enrollment in Part BCMS-40B. The government provides a slightly different form to individuals with this coverage which can include Medicare Part A Medicare Advantage Medicaid CHIP Tricare and more. People with Medicare who want to join a Medicare Advantage Plan To join a plan you must.
If you dont have standard identity documents you can use a referee instead. If you worked for a railroad call the Railroad Retirement Board at 1-877-772-5772 TTY users. If you already have Medicare Part B skip to step 3.
You can also apply online at the Social Security website and fill out the Medicare application form or visit your local Social Security office in person and complete your Medicare enrollment form there. You know you have Part B if you have a red white and blue Medicare card that says Medical Part B You will use that card as proof of Medicare enrollment. Part B document 40B.
To join a Medicare Advantage Plan.