The form CMS-L458 is a notice from the Centers for Medicare Medicaid Services that your Part A hospital insurance will end per your request The form CMS-L458 is a notice from the Centers for Medicare Medicaid Services that your Part A hospital insurance will end per your request. The following form should be completed by individuals who have become eligible for Medicaid benefits because they are in receipt of Supplemental Security Income andor State Supplement Program benefits.
Https Www Health Ny Gov Forms Doh 5178a Dd Access Pdf
Proof of age birth certificate or drivers license.

Medicaid supplement a form. Expand I have Part A and want to apply for Part B Application for Enrollment in Part BCMS-40B. Medicare Supplement also known as Medigap is a category of Medicare insurance products offered by private insurance companies. NEW SUPPLEMENT A FORM DOH-5178A.
Your banking information and a voided check if you want to sign up for automatic payment withdrawal. Medigap plans are designed to work with Original Medicare and they can close some or all of the gaps in your Original Medicare coverage. If you are applying for the Medicare Savings Program MSP only this Supplement does not need to be completed.
Helps with medical costs for some people with limited income and resources Offers benefits not normally covered by Medicare like nursing home care and personal care services How to apply for Medicaid Each state has different rules about eligibility and applying for Medicaid. The form should be returned to your Local District Social Services Offices. It could be because they are new to your market and want to buy your business.
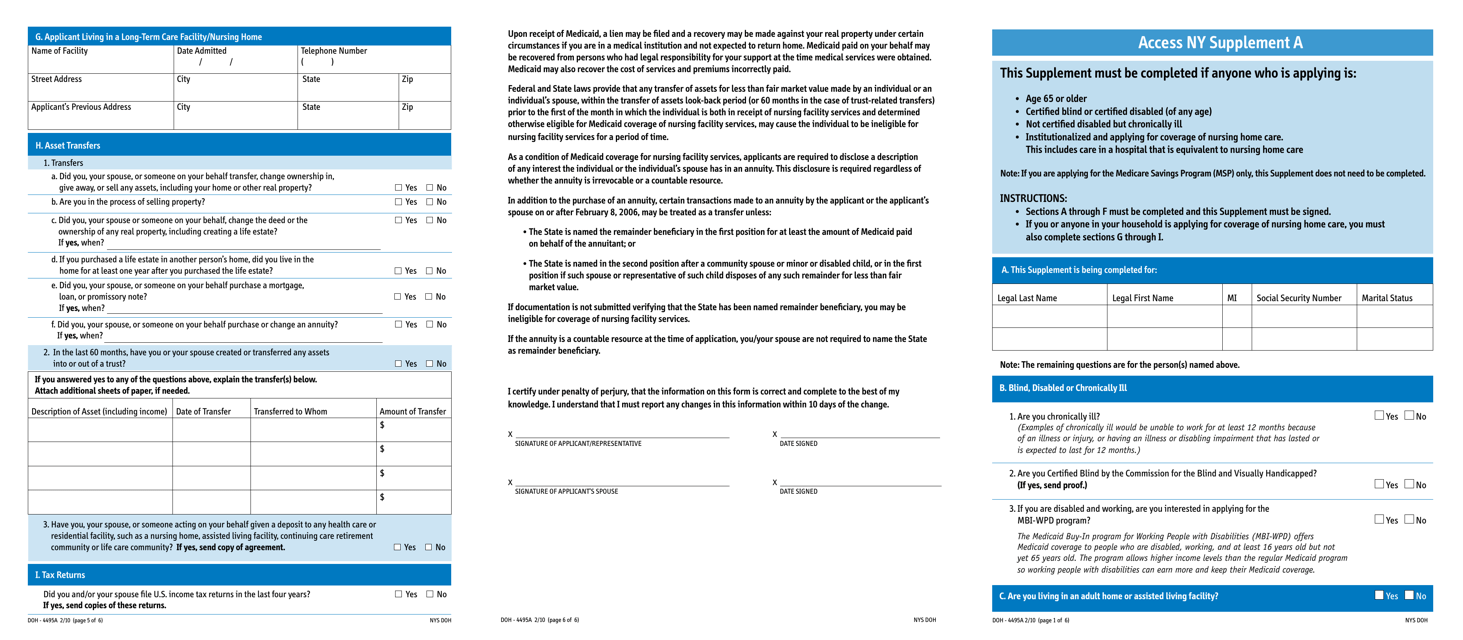
Access NY Supplement A This Supplement must be completed if anyone who is applying is. These documents contain information about your benefits network and coverage. Fill out the Authorization Agreement for Pre-authorized Payments form SF-5510 as a PDF in English or HTML in English.
Before you submit your Medicaid application be sure to have all of the following documentation ready. 2021 Medicare Supplement Outline of Coverage PDF 2021 Medicare Supplement Application Form PDF 2021 Medicare Supplement Dental Vision Hearing Application Form PDF. All You Need To Achieve Your Goals Is Right Here At Myprotein - Order Online.
PMS- 022 D Med Supp Application MDS-002 Providence Medicare Supplement Application 9 Please review the following information about Medicare Supplement policies You do not need more than one Medicare Supplement policy. For those age 65 or who are disabled or blind a second form is also required - Supplement A - As of Jan. Get the SF-5510 as a PDF form in Spanish or HMTL form in Spanish.
The form and the entire Medicaid application can also be found in various languages at httpswwwhealthnygovhealth_caremedicaid. 2021 the same Supplement A form. Yes in the states of New York and California the cost of Medicare supplement insurance also called MediGap premiums can be used to reduce ones monthly income to meet Medicaids income limit and hence gain Medicaid eligibility.
Supplement A Supplement to Access NY Health Care Application DOH-4220 This Supplement must be completed if anyone who is applying is. Sections A through F must be completed and this Supplement must be signed. If you or anyone in your household is applying for coverage of nursing home care you must also complete sections G through I.
This strategy may also potentially be used in one or two other states but at the time of this writing it is undetermined if this is. Supplement A Supplement to Access NY Health Care Application DOH-4220 This Supplement must be completed if anyone who is applying is. Ad Explore The Range Of Premium Quality Supplements At Europes No1 Sports Nutrition Brand.
Use DOH-5178A - the same form that has been used outside of NYC. If you see a cheap price on a Medicare Supplement Plan. Dont get trapped in their marketing because they could raise your rate significantly in the future.
Call your state Medicaid program to see if you. By Valerie Bogart New York Legal Assistance Group Since 2010 the New York State Department of Health Medicaid application form is called the Access NY Application or form DOH-4220. Gather all necessary information to fill out the Medicaid application.
What youll need to apply. Sections A through F must be completed and this Supplement must be signed. DO NOT USE Form DOH-4495A which has been used in NYC until now.
Download the form at this link As of January 2021 the form was last updated in March 2015. The notice will state the date your coverage will end and provide you with the opportunity to change. Use these forms if youd like BlueCross to accept bank draft payments.
Medicaid is a joint federal and state program that. Your Social Security number. Age 65 or older Certified blind or certified disabled of any age Not certified disabled but chronically ill Institutionalized and applying for coverage of nursing home care.
Medicaid applications are often denied because of incomplete information on the application form. Medicare Supplement is also known as BlueElite SM and should be listed on your Member ID card. So basically just because its cheap now does not mean that you made a good long term decision.
Age 65 or older Certiied blind or certiied disabled of any age Not certiied disabled but chronically ill Institutionalized and applying for coverage of nursing home care. If you purchase this policy you may want to evaluate your existing health coverage and decide if you need multiple coverage. Upon receipt of Medicaid a lien may be iled and a recovery may be made against your real property under certain StreetAddress.
Https Www Finaid Wwu Edu Client Services Media Pdfs Online Forms B General Processing Forms Medicaid Ssi Verification Parent Pdf
Https Www1 Nyc Gov Assets Hra Downloads Pdf Services Micsa Hcsp 3052 20immediate 20need 20transmittal Pdf
Http Www Wnylc Com Health File 449
Https Rappslaw Com Wp Content Uploads 2015 02 Ny Medicaid Application Pdf
Https Rappslaw Com Wp Content Uploads 2015 02 Ny Medicaid Application Pdf
Https Www Dhs Wisconsin Gov Forms F02520 Pdf
Fillable Online Healthandwelfare Idaho Idaho Medicaid Sgd Supplemental Form Please Complete Entire Fax Email Print Pdffiller
 Form Doh 4495a Supplement A Download Printable Pdf Or Fill Online Access Ny New York Templateroller
Form Doh 4495a Supplement A Download Printable Pdf Or Fill Online Access Ny New York Templateroller
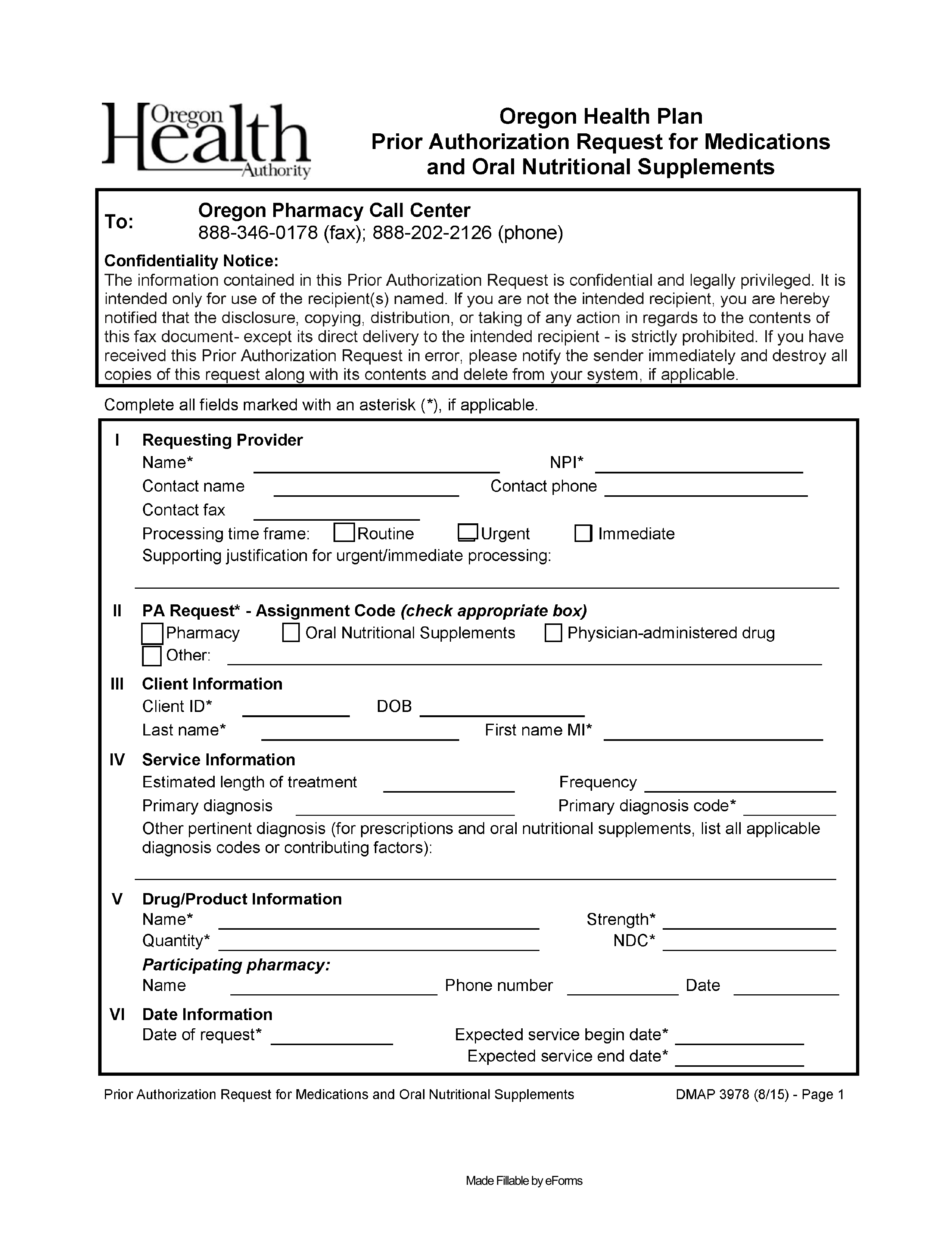 Free Oregon Medicaid Prior Authorization Form Pdf Eforms
Free Oregon Medicaid Prior Authorization Form Pdf Eforms
Https Rappslaw Com Wp Content Uploads 2015 02 Ny Medicaid Application Pdf
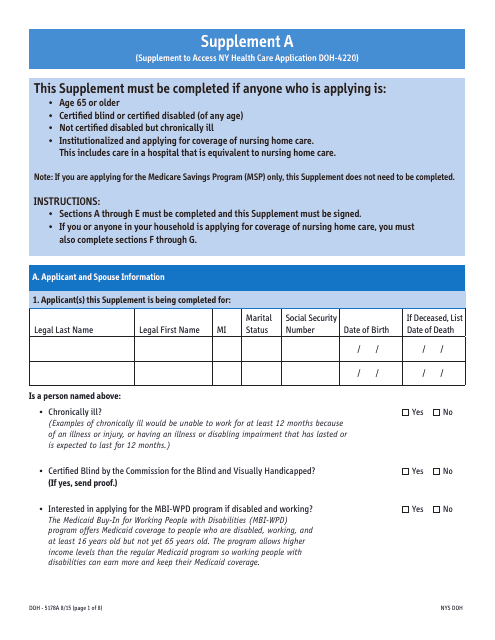 Form Doh 5178a Supplement A Download Printable Pdf Or Fill Online Supplement To Access Ny Health Care Application Doh 4220 New York Templateroller
Form Doh 5178a Supplement A Download Printable Pdf Or Fill Online Supplement To Access Ny Health Care Application Doh 4220 New York Templateroller
Https Www Qhpcertification Cms Gov S Data Change Worksheet Sup A Py2018 Pdf V 1
N Y M E D I C A I D S U P P L E M E N T A F O R M Zonealarm Results
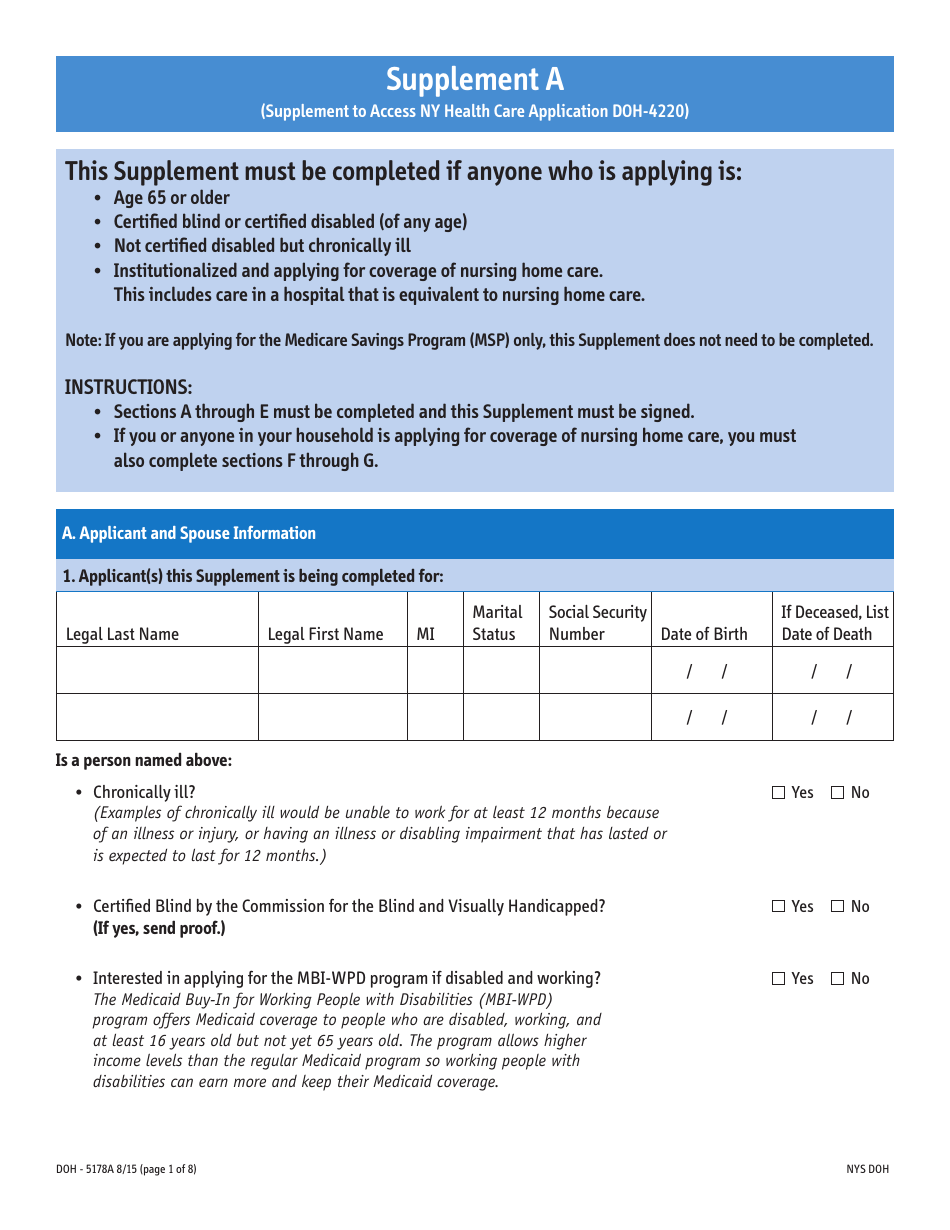 Form Doh 5178a Supplement A Download Printable Pdf Or Fill Online Supplement To Access Ny Health Care Application Doh 4220 New York Templateroller
Form Doh 5178a Supplement A Download Printable Pdf Or Fill Online Supplement To Access Ny Health Care Application Doh 4220 New York Templateroller
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.