Allow at least 24 hours for review. 33 Zeilen Form 471.
 Priority Health Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
Priority Health Prior Authorization Form Fill Online Printable Fillable Blank Pdffiller
If you are unable to locate a specific drug on our formulary you can also select Non-Formulary Medications then complete and submit that prior authorization form.

Medication prior authorization form. FORMS ARE UPDATED FREQUENTLY AND MAY BE BARCODED Patient Information required Provider Information required Patient Name. Medica Care Management Route CP440 PO Box. Medication Prior Authorization Form Author.
1-800-689-2759 Hoosier Healthwiseauthorize the Anthem Hoosier Healthwise P. Medication PA prior authorization California Created Date. Pharmacy Prior Authorization Forms Preferred Drug List Health Resources.
MASSACHUSETTS STANDARD FORM FOR MEDICATION PRIOR AUTHORIZATION REQUESTS Some plans might not accept this form for Medicare or Medicaid requests. If you have questions please call 800-310-6826. The Medicaid prior authorization forms appeal to the specific State to see if a drug is approved under their coverage.
1-800-457-4584 option 7 F. Prior Authorization Change Request NOT to be used for Pharmacy prior. Prescription prior authorization forms are used by physicians who wish to request insurance coverage for non-preferred prescriptions.
Download and print the form for your drug. Prior Authorization Request Form Please complete this entire form and fax it to. For Part D prior authorization forms please see the Medicare section.
Please include ALL pertinent clinical information with your Medical or Pharmacy Prior Authorization request submission. This form is being used for. You dont need to send multiple forms.
If you require a prior authorization for a medication not listed here please contact UPMC Health Plan Pharmacy Services at 1-800-979-UPMC 8762. Prior Authorization Request Form DO NOT COPY FOR FUTURE USE. Use the Online Prior Authorization and Notification tool KanCare Medicaid Behavioral Health Inpatient Prior Authorization Request Form.
To ensure that prior authorizations are reviewed promptly submit request with. Massachusetts Commercial Prior Authorization Form - Cardiac Imaging Prior Authorization Form. Forms used in PA Unit include the following.
Initial Request ContinuationRenewal Request Reason for request check all that apply. Member Information Prescriber Information Member Name. IHCP Prior Authorization Request Form Version 62 May 2021 Page 1 of 1 Indiana Health Coverage Programs Prior Authorization Request Form Fee-for-Service Gainwell Technologies P.
This form may contain multiple pages. Puerto Rico prior authorization. Forms for state mandates.
A request must be submitted and approved in advance for medications. A medication prior authorization form. Prior Authorization Forms The Prior Authorization PA unit at AHCCCS authorizes specific services prior to delivery of medical related services.
Please complete all pages to avoid a delay in our decision. Prior Authorization Step Therapy Formulary Exception. Search for your drug on the TRICARE Formulary Search Tool.
Your authorization approval will apply to network pharmacies and home delivery. If the patient has tried any preferred medications. Prior Authorizations Forms.
Complete the applicable form below and fax it to 1-855-681-8650. PA request status can be viewed online. Authorized Representative Request PDF Medicare Member Authorization Appeal-appealing Medicare denials of medical prior authorization precertification requests PDF Medicare Non-contracted Provider Appeal Process PDF Medicare Appeals Provider Memo- Post Service PDF.
This form is to be completed by the patients medical office to see if he or she qualifies under their specific diagnosis and why the drug should be used over another type of medication. Faxing 952-992-3556 or 952-992-3554. Cant Find a Form.
To begin the prior authorization process providers may submit prior authorization requests to Medica Care Management by. Instructions are on the form. A non-preferred drug is a drug that is not listed on the Preferred Drug List PDL of a given insurance provider or State.
Medication ExceptionPrior Authorization Request Form Fax this form and supporting chart notes to 503 346-8351 For questions contact OHSU PBM Services at 844-827-6572. Sending an electronic Prior Authorization Form. Give the form to your provider to complete and send back to Express Scripts.
How to Get Prior Authorization. On the prior authorization form the person making the request must provide a medical rationale as to why the chosen medication is necessary for the patient in question. KanCare Medicaid Behavioral Health PRTF Prior Authorization Request Form.
Prior authorization for pharmacy drugs Submitting a request for prior authorization.
 Free 9 Sample Prior Authorization Forms In Ms Word Pdf
Free 9 Sample Prior Authorization Forms In Ms Word Pdf
 Optumrx Prior Authorization Form Fill Out And Sign Printable Pdf Template Signnow
Optumrx Prior Authorization Form Fill Out And Sign Printable Pdf Template Signnow
Https Www Lacare Org Sites Default Files Prescription Prior Authorization Request Form Medi Cal Pdf
 Surescripts Medication Prior Authorization Form Pdf Fill Online Printable Fillable Blank Pdffiller
Surescripts Medication Prior Authorization Form Pdf Fill Online Printable Fillable Blank Pdffiller
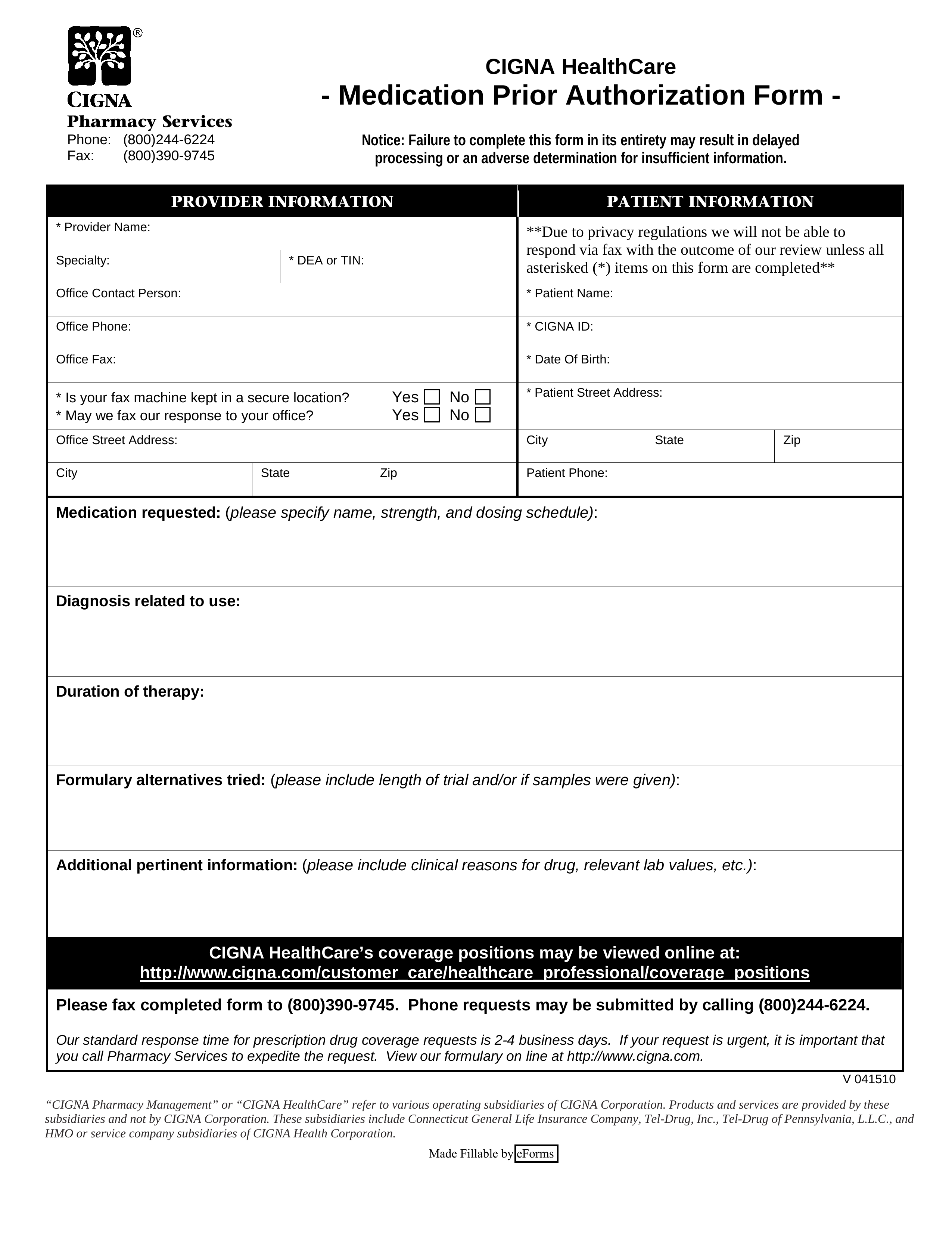 Free Cigna Prior Rx Authorization Form Pdf Eforms
Free Cigna Prior Rx Authorization Form Pdf Eforms
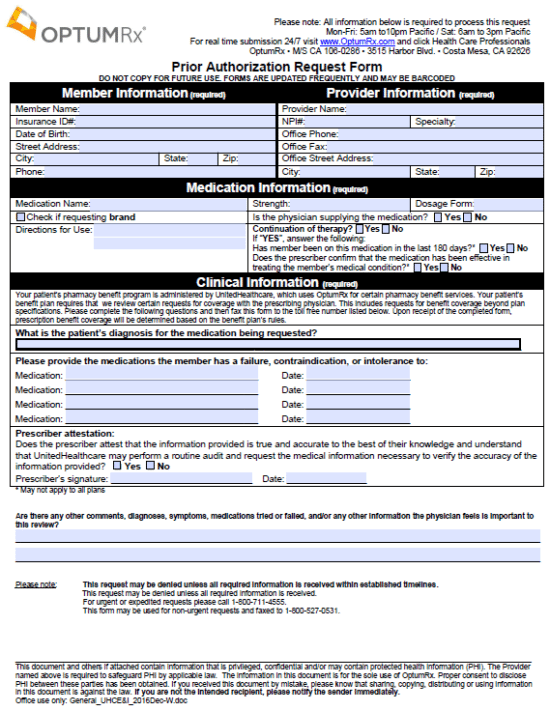 Optumrx Prior Prescription Rx Authorization Form Authorization Forms
Optumrx Prior Prescription Rx Authorization Form Authorization Forms
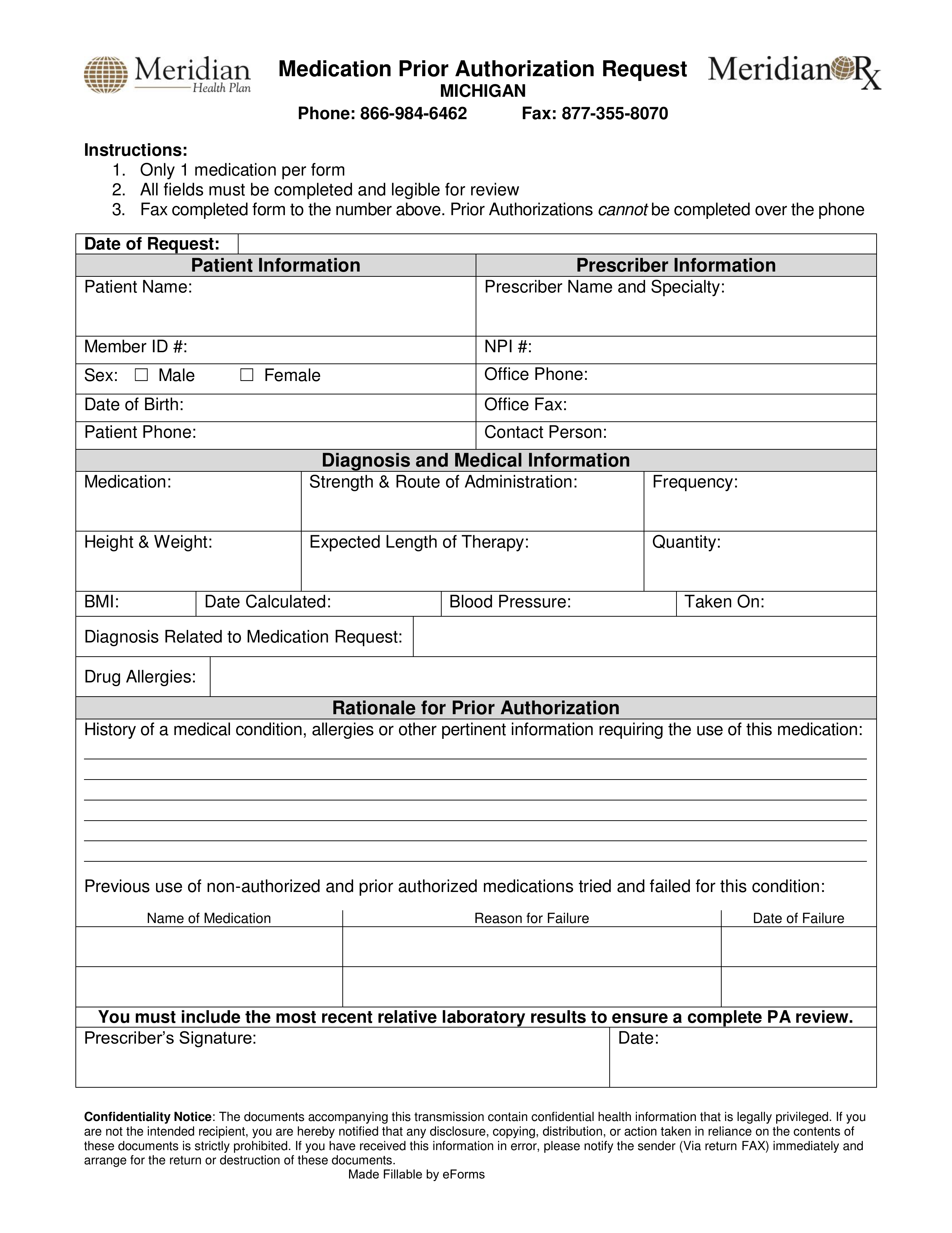 Free Meridian Prior Rx Authorization Form Pdf Eforms
Free Meridian Prior Rx Authorization Form Pdf Eforms
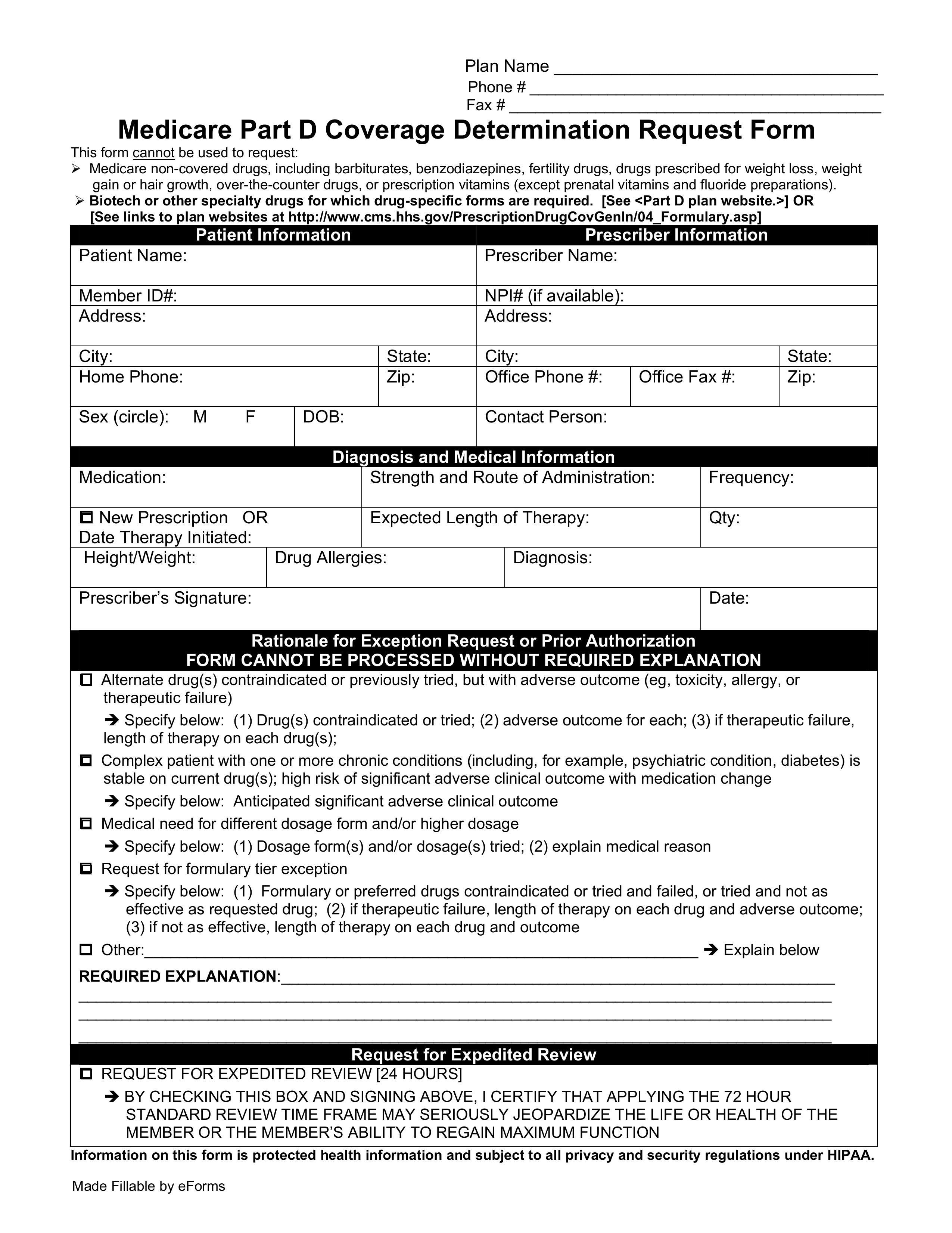 Free Medicare Prior Rx Authorization Form Pdf Eforms
Free Medicare Prior Rx Authorization Form Pdf Eforms
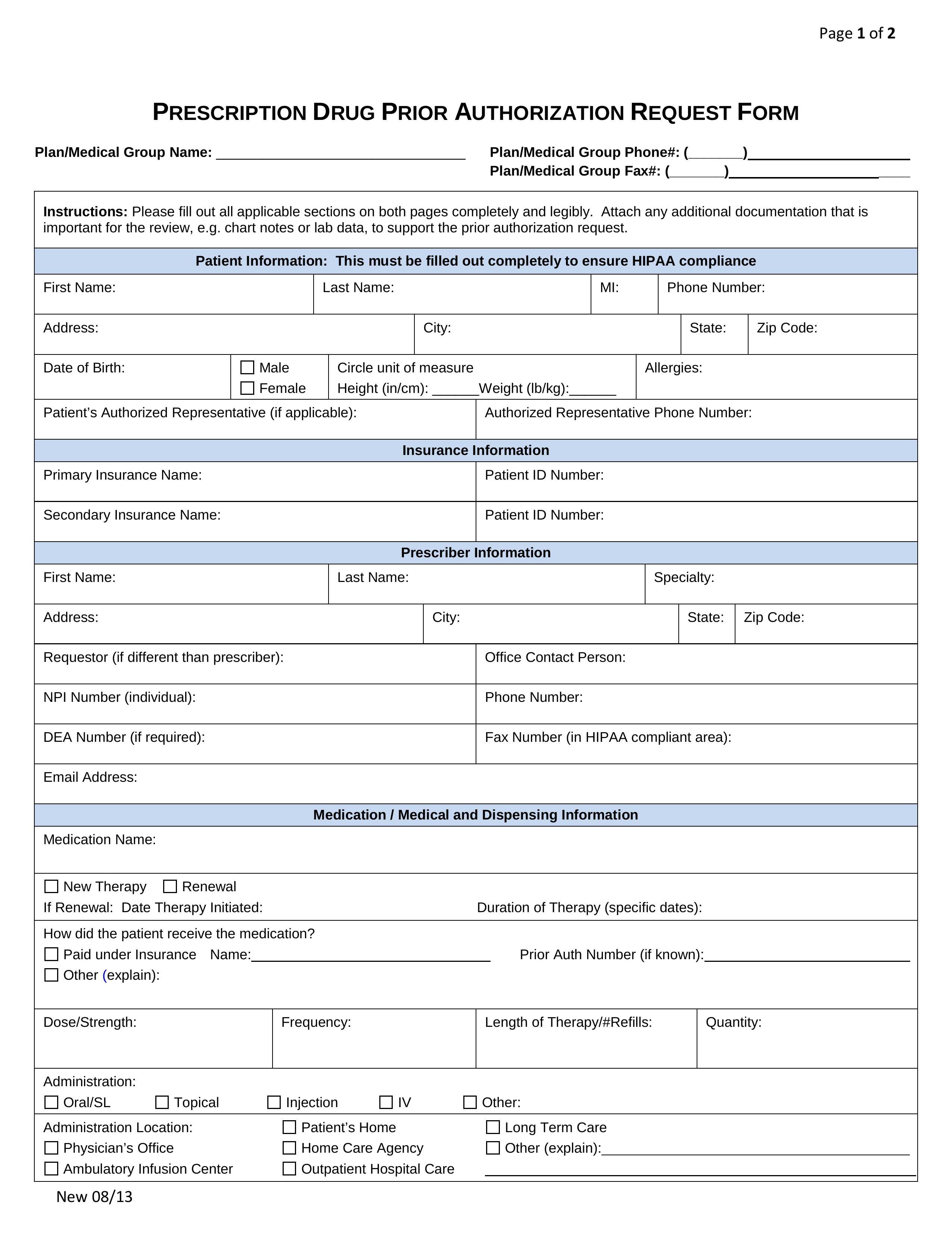 Free Prior Rx Authorization Forms Pdf Eforms
Free Prior Rx Authorization Forms Pdf Eforms
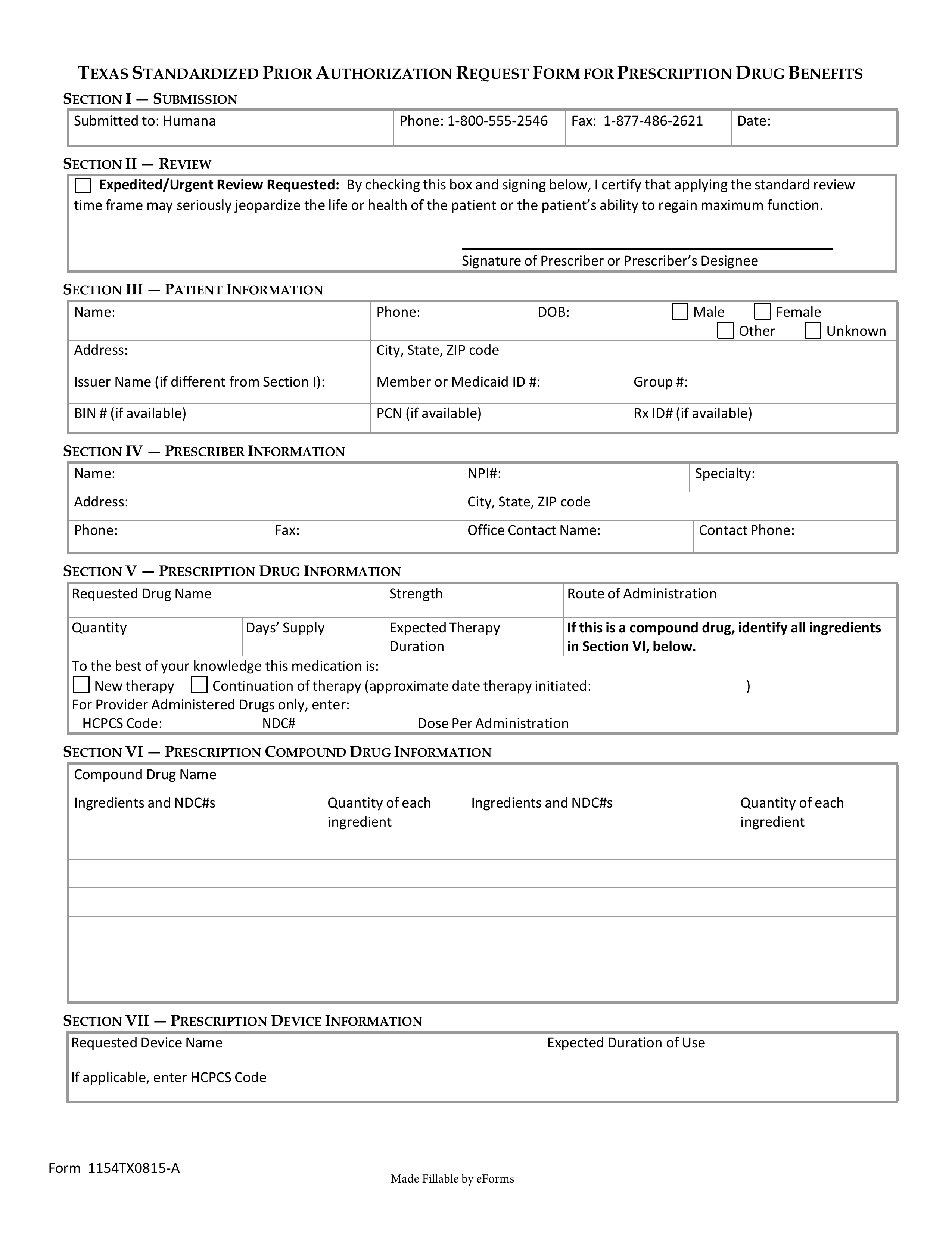 Free Humana Prior Rx Authorization Form Pdf Eforms
Free Humana Prior Rx Authorization Form Pdf Eforms
Fillable Online Medication Prior Authorization Form Fax Back To 18775779045 Member Information Last Name Phone 18775779044 D Fax Email Print Pdffiller
 Cigna Prior Prescription Rx Authorization Form Authorization Forms
Cigna Prior Prescription Rx Authorization Form Authorization Forms
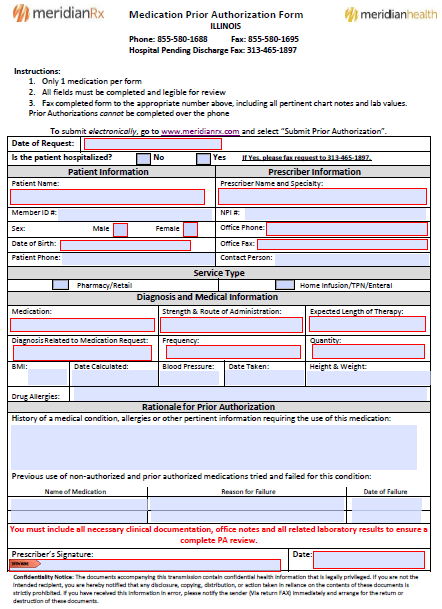 Meridian Prior Prescription Rx Authorization Form Authorization Forms
Meridian Prior Prescription Rx Authorization Form Authorization Forms
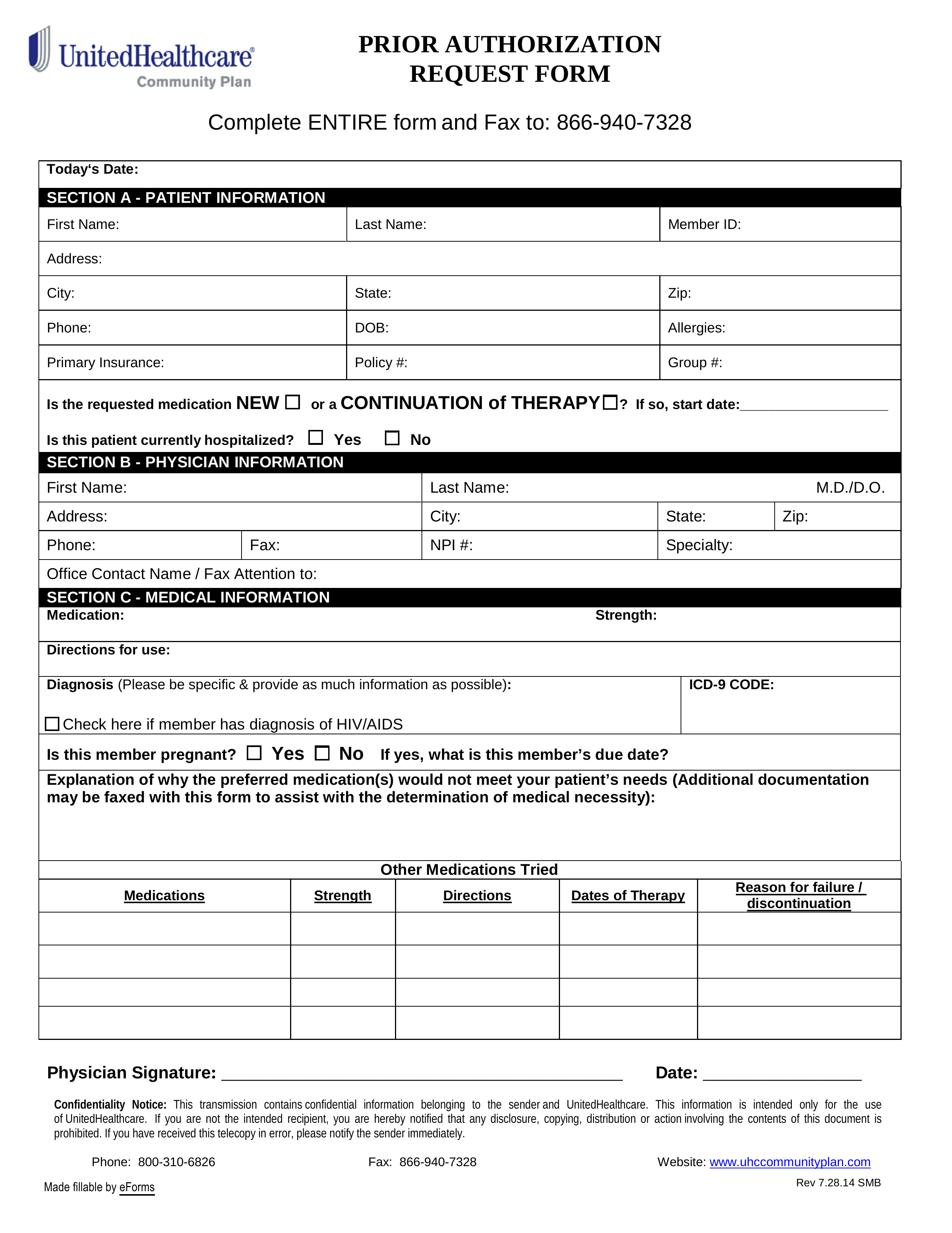 Free Unitedhealthcare Prior Rx Authorization Form Pdf Eforms
Free Unitedhealthcare Prior Rx Authorization Form Pdf Eforms
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.