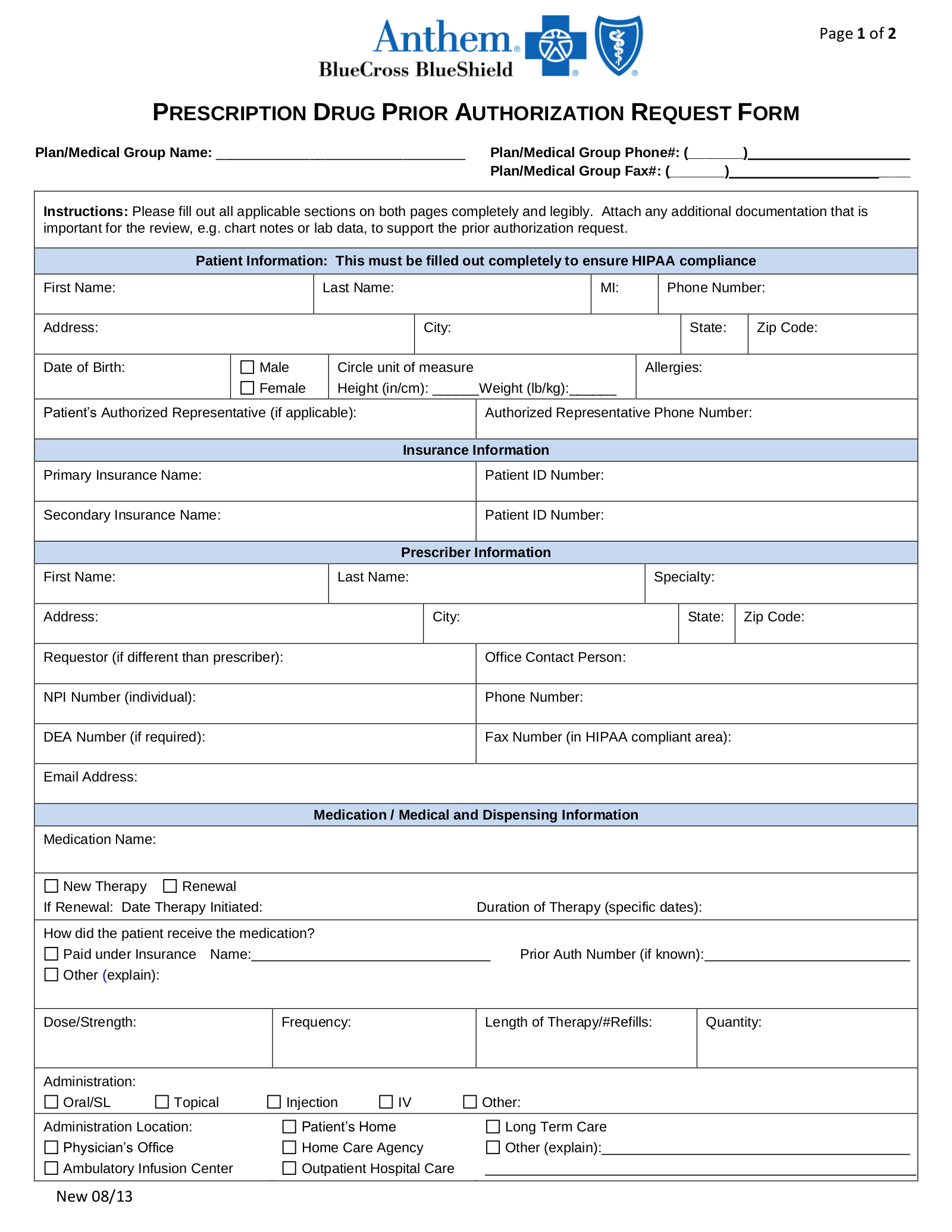
Prescription prior authorization forms are used by physicians who wish to request insurance coverage for non-preferred prescriptionsA non-preferred drug is a drug that is not listed on the Preferred Drug List PDL of a given insurance provider or State. To enroll reenroll or to elect not to enroll in the FEHB Program or to change cancel or suspend your FEHB enrollment please complete and file this form.
 F E P P R I O R A U T H O R I Z A T I O N F O R M Zonealarm Results
F E P P R I O R A U T H O R I Z A T I O N F O R M Zonealarm Results
Clinical Services 1-877-378-4727 R.
Fep prior authorization form. Attached is a Prior Authorization request form. Box 52080 MC 139 Phoenix AZ 85072-2080 Attn. FEP fax cover sheet- Include this cover sheet when submitting a corrected claim mailing or faxing medical records for a claim or submitting an appeal.
To give prior approval we need to confirm two things. Standard and Basic Option prior approval list FEP Blue Focus prior approval list. For your convenience there are 3 ways to complete a Prior Authorization request.
Service Benefit Plan Prior Approval PO. Otezla FEP MD Fax Form Revised 112021 Send completed form to. Box 52080 MC 139 Phoenix AZ 85072-2080 Attn.
Prior authorization must be obtained prior to the delivery of. Patient Information required Provider Information required Date. Authorized Representative Designation Form.
Service Benefit Plan Prior Approval PO. Botox FEP MD Fax Form Revised 352021 Send completed form to. BCBSTX 1-800-528-7264 Refer to the online Blue Choice PPO Provider Manual Section I for more detailed information.
Box 52080 MC 139 Phoenix AZ 85072-2080 Attn. Find forms for Blue Shield Promise Medi-Cal and Cal MediConnect members. On the prior authorization form the person making the request must provide a medical rationale as to why the chosen medication is necessary.
For your convenience there are 3 ways to complete a Prior Authorization request. Service Benefit Plan Prior Approval PO. Find forms you may need to submit prior authorization requests.
FEP PPO PRESCRIPTION DRUG PRIOR AUTHORIZATION OR STEP THERAPY EXCEPTION REQUEST FORM PlanMedical Group Name. Attached is a Prior Authorization request form. Send completed form to.
Service Benefit Plan Prior Approval PO. Attached is a Prior Authorization request form. Box 52080 MC 139 Phoenix AZ 85072-2080 Attn.
Service Benefit Plan Prior Approval PO. To request prior approval or to obtain a list of drugs and supplies that require prior approval call CVS Caremark FEPs pharmacy program admin istrator at 877-727-3784 from 7. Find forms for Blue Shield IFP Small Large Group and Medicare members.
Patient Information required Provider Information required Date. Repatha FEP MD Fax Form Revised 352021 Send completed form to. That youre using the drug to treat something we cover and that your healthcare provider prescribes it in a medically appropriate way.
Prior approvalpre-service request forms for services provided in Alaska or Washington only. In some situations you need to get your care treatment. However some select drugs require your doctor to provide information about your prescription to determine coverage.
Methylphenidate FEP MD Fax Form Revised 422021 Send completed form to. Box 52080 MC 139 Phoenix AZ 85072-2080 Attn. PPI FEP MD Fax Form Revised 112021 Send completed form to.
You can see the full list of prescription drugs that need to be approved here. Most drugs are covered without requiring prior approval. Electronically Online ePA Results in 2-3 minutes.
Blue Shield of California Non-Urgent- The Federal Employee Program has a 15 Day turn-around time on all Prior Authorization Requests according to the Blue Cross Blue Shield Service Benefit Plan. Service Benefit Plan Prior Approval PO. Use this form to select an individual or entity to act on.
IR Opioid Combo FEP MD Fax Form Revised 412021 Send completed form to. Provided herein is not sufficient to make a benefit determination or requires clarification and I agree to provide any such information to the insurer. FEP will waive prior authorizations for medically necessary diagnostic tests and covered services that are consistent with CDC guidance if diagnosed with COVID-19.
For your convenience there are 3 ways to complete a Prior Authorization request. Incident questionnaire - Submit this form if you or a covered dependent has an injury or if a claim is pending for this information. Your healthcare provider can request prior approval electronically by fax or by mail.
To obtain prior authorization call. 1-877-378-4727 R the physician portion and submit this completed form. Box 52080 MC 139 Phoenix AZ 85072-2080 Attn.
Prior authorization is required from BCBSTX for all inpatient partial hospitalization and outpatient behavioral health services. Box 52080 MC 139 Phoenix AZ 85072-2080 Attn. For durable medical equipment DME prior approvals.
1-877-378-4727 R the physician portion and submit this completed form. Service Benefit Plan Prior Approval PO. Clinical Services 1-877-378-4727 R.
Health Benefits Election Form SF 2809 Form To enroll reenroll or to elect not to enroll in the FEHB Program or to change cancel or suspend your FEHB enrollment please complete and file this form. Alaska DME prior approval form Washington DME prior approval form. Drug prior approval is a process to obtain advanced approval of coverage for a prescription drug.
Provided herein is not sufficient to make a benefit determination or requires clarification and I agree to provide any such information to the insurer. View Blue Shield and FEP Prior Authorization list PDF 178 KB Prior authorization forms. Alaska prior approval form Washington prior approval form.