Massachusetts Standard Form for Medication Prior Authorization Requests eForm or contact Clinical Pharmacy Operations. Blue Cross Blue Shield of Michigan and Blue Care Network.
Https Bluecrossnc Com Sites Default Files Document Attachment Common Pdfs Hmo Ppo General Quantity Limitations Fax Request Form Pdf
Has the requested drug been dispensed at a pharmacy and approved for coverage previously by a prior plan.
Bcbs pharmacy prior authorization form. Prior Authorization Health insurance can be complicatedespecially when it comes to prior authorization also referred to as pre-approval pre-authorization and pre-certification. Important for the review eg. To request prior authorization for these medications please submit the.
Health Care Proxy Form The New York Health Care Proxy Law allows you to appoint someone you trust to make health care decisions for you if you lose the ability to make decisions yourself. Form Title Networks Expedited Pre-service Clinical Appeal Form. Initial Request C o n tinua R ewal R ques Reason for request check all that apply.
Contact person for this. For expedited authorization codes call Premera pharmacy services at 888-261-1756. Submit an electronic prior authorization request.
A prior authorization is not a guarantee of. Medicaid Claims Inquiry or Dispute Request Form. Information contained in this form is Protected Health Information under HIPAA.
Other medications that require prior authorization. Blue Choice members using their self-referred benefit do not need to get prior authorization. ANTHEM is a registered trademark of Anthem Insurance Companies Inc.
Yes or No. Complete this form in its entirety. Drug Prior Authorization Request Form.
Opioid attestation Specific to School Employees Benefits Board SEBB members undergoing active cancer treatment hospice palliative care end-of-life or medically necessary care who might be exempt from quantity limits. Is an independent licensee of the Blue Cross and Blue Shield Association. HFS 3082 R-12-11 DOB.
You or your physician should fax the completed form to FutureScripts at 1-888-671-5285 for review. Chart notes or lab data to support the prior authorization or step-therapy exception request. Blue Advantage Drug Coverage Determination Formulary or Tier Exception Drug Authorization Forms Quantity Limit Drug Authorization Forms and Step Therapy Drug Authorization Forms.
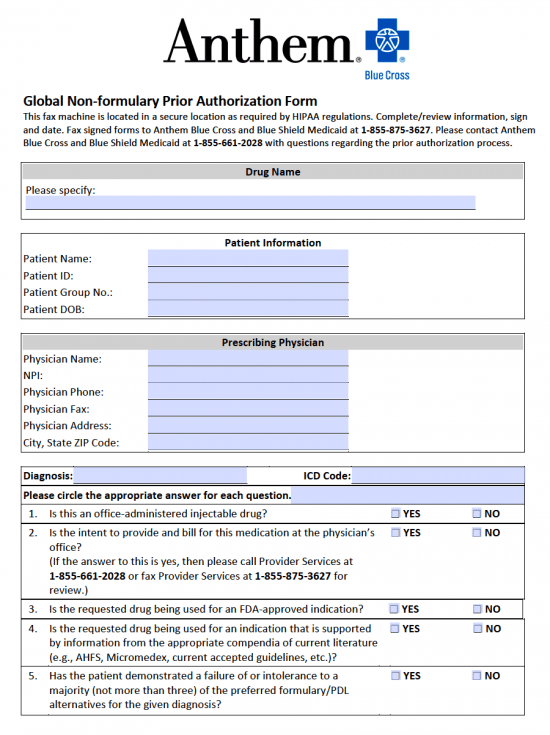
Nine-Digit HFS Recipient. The form contains important information regarding the patients medical history and requested medication which Anthem will use to determine whether or not the prescription is included in the patients health care plan. Acute Inpatient Fax Assessment Form PDF Acute Rehabilitation and Skilled Nursing Facility Assessment Form PDF Benefit Enhancement Assessment Form PDF LTACH and Skilled Nursing Facility Enhancement Assessment Form PDF Blue Cross PPO Request for Preauthorization Form.
This form is being used for. Weve provided the following resources to help you understand Empires prior authorization process and obtain authorization for your patients when its required. Or download the PA and ST program criteria summaries and fax forms from the Prime Therapeutics website using the following links.
Prior authorization is required for some membersservicesdrugs before services are rendered to confirm medical necessity as defined by the members health benefit plan. Durable Medical Equipment Preauth form This form is used to request a Prior Authorization for Durable Medical Equipment DME. Some drugs on the drug list require prior authorization and certain clinical criteria must be met before they can be dispensed.
The Anthem Blue Cross Blue Shield prior authorization form is what physicians will use when requesting payment for a patients prescription cost. Prior authorization sometimes called preauthorization or pre-certification is a pre-service utilization management review. Formulary ExceptionPrior Authorization Request Form Patient Information Prescriber Information Patient Name.
Room Rate Update Notification. Pharmacy information required only when pharmacy is the requesting provider. Office drugs prior authorization request PDF 301 KB.
Physicians can access complete and submit PA and ST program criteria summaries and request forms electronically from the CoverMyMeds website. MASSACHUSETTS STANDARD FORM FOR MEDICATION PRIOR AUTHORIZATION REQUESTS Some plans might not accept this form for Medicare or Medicaid requests. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form.
Blue Cross Medical Record Routing Form PDF Commercial. Prior AuthorizationCoverage Determination Form PDF 136 KB Prior Authorization Generic Fax Form PDF 173 KB Prior Authorization Urgent Expedited Fax Form PDF 126 KB Tier Exception PDF 109 KB Prescription drug prior authorization and step therapy exception request forms. Patient Information First Name.
BlueRx Drug Prior Authorization. If you have not received a response after two business days from when your completed form was submitted please contact the physician who requested your prior authorization. Prior Authorization Step Therapy Formulary Exception.
Other drugs are part of our step-therapy program which means the patient must be treated with one or more preferred drug therapies before these drugs are covered. Take the appropriate request form to your physician for completion. AVAPEC-1601-17 December 2017 Instructions.
Blue Advantage Drug Prior Authorization. Please provide dosage form. Blue Advantage Physician Drug Authorization Request Form.
Home Health Care Preauthorization Form. Out-of-Network Enrollee Notification Form for Non-Regulated Business Use this form if TDI is not on members ID card PPO Notification for non pre-cert surgeries per Texas Administrative Code 33703. Medicaid only BCCHP and MMAI.